

Tesamorelin for Visceral Fat Studies: A 2026 Scientific Research Review
- peptideresearchau
- 1 day ago
- 12 min read

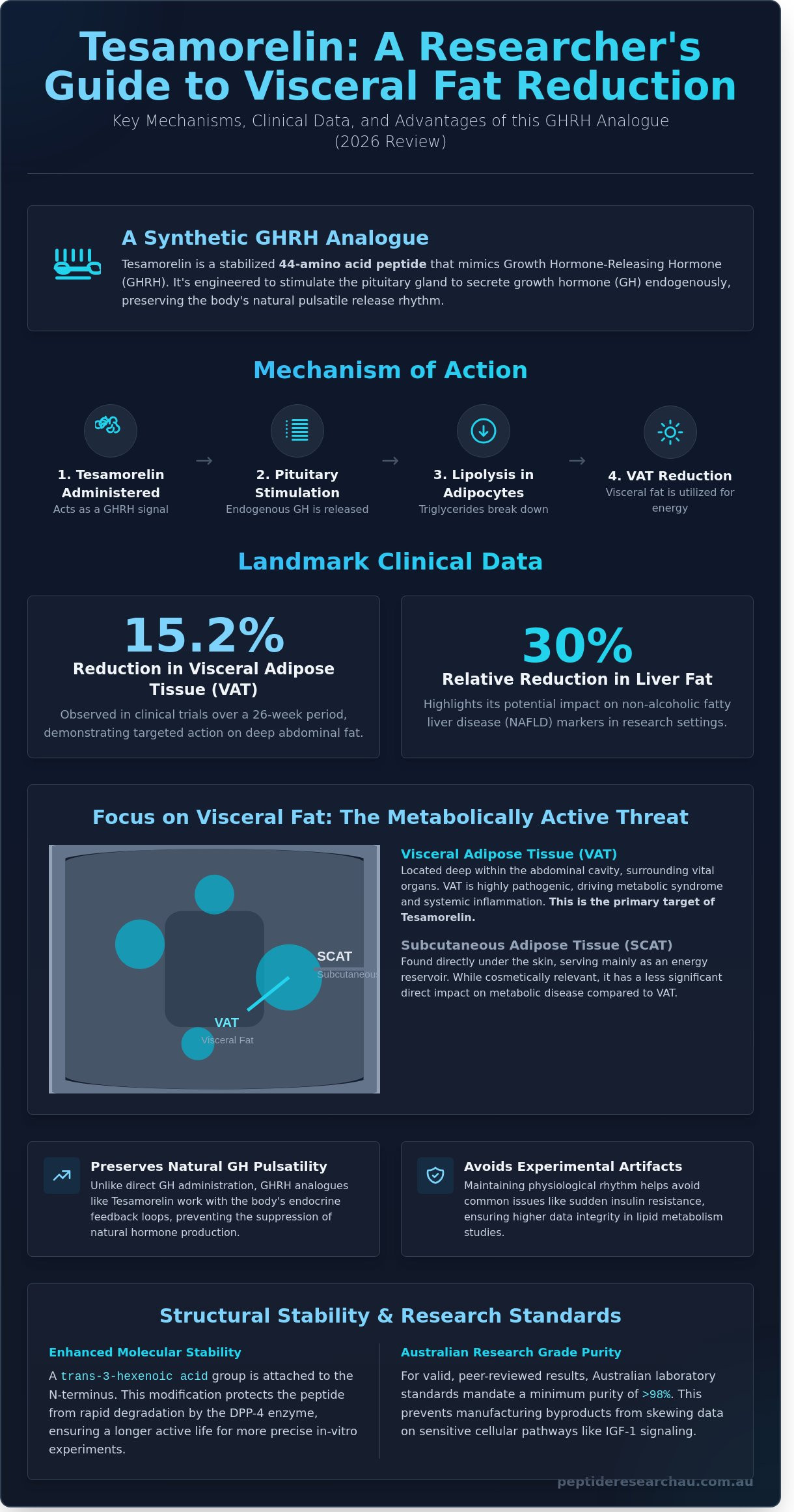
Did you know that clinical trials involving Tesamorelin demonstrated a 15.2% reduction in visceral adipose tissue (VAT) within just 26 weeks? For researchers in Australia, identifying compounds that specifically target deep abdominal fat without the systemic side effects of generic growth hormone is a common challenge. You likely recognize that visceral fat isn't just a cosmetic issue; it's a metabolic driver of chronic disease. This 2026 review synthesizes the latest tesamorelin for visceral fat studies to provide clarity on its unique Growth Hormone Releasing Hormone (GHRH) mechanism and its impact on non-alcoholic fatty liver disease (NAFLD).
We'll provide a comprehensive analysis of significant VAT reduction statistics and the biochemical pathways that differentiate this peptide from standard GH therapies. You'll also find a precise protocol for laboratory reconstitution and insights into sourcing laboratory-grade compounds within the Australian regulatory framework. From its 44-amino acid structure to its documented effect on liver fat, this guide serves as your authoritative resource for modern peptide research.
Key Takeaways
Understand the biochemical mechanism of Tesamorelin as a synthetic GHRH analogue and its role in stimulating endogenous growth hormone production within laboratory settings.
Differentiate between Visceral Adipose Tissue (VAT) and Subcutaneous Adipose Tissue (SCAT) to identify why VAT is the primary driver of metabolic research outcomes.
Analyze landmark clinical data demonstrating a statistically significant 30% relative reduction in liver fat, providing a foundation for tesamorelin for visceral fat studies.
Evaluate the comparative efficacy of Tesamorelin against other research-grade secretagogues like Ipamorelin and CJC-1295 for targeted adipose tissue reduction.
Master essential laboratory protocols for the reconstitution and temperature-controlled storage of lyophilized peptides to ensure the integrity of your research compounds.
Table of Contents Understanding Tesamorelin: A Growth Hormone-Releasing Hormone (GHRH) Analogue The Pathophysiology of Visceral Adipose Tissue (VAT) in Metabolic Research Key Clinical Studies: Tesamorelin’s Impact on Visceral Fat and Liver Health Comparative Analysis: Tesamorelin vs. Other Growth Hormone Secretagogues Laboratory Protocols: Reconstitution and Handling of Tesamorelin
Understanding Tesamorelin: A Growth Hormone-Releasing Hormone (GHRH) Analogue
Tesamorelin is a synthetic peptide consisting of a 44-amino acid sequence. It functions as a Growth Hormone-Releasing Hormone (GHRH) analogue, specifically designed to stimulate the endogenous production of growth hormone. Modern applications of tesamorelin for visceral fat studies focus on its ability to target ectopic fat depots without the systemic complications often seen with direct hormone replacement. Researchers value this compound because it prompts the pituitary gland to secrete growth hormone in a controlled manner rather than introducing exogenous hormones into a biological system.
This distinction is critical for data integrity in laboratory settings. Direct growth hormone administration often suppresses the natural endocrine feedback loops. In contrast, GHRH analogues are preferred in research because they maintain natural GH pulsatility. Preserving this physiological rhythm helps avoid common experimental artifacts like sudden insulin resistance. Maintaining this natural rhythm allows for a more accurate assessment of how the peptide influences lipid metabolism over extended 2026 trial periods.
The stability of this peptide is enhanced by a specific N-terminal modification. By attaching a trans-3-hexenoic acid moiety to the N-terminus, scientists have created a version that resists enzymatic degradation by dipeptidyl peptidase IV. This structural change ensures the compound remains active longer during in vitro experiments. It allows for more precise observations of hormonal interactions over 24-hour cycles without the rapid breakdown seen in unmodified GHRH(1-44)amide.
The Mechanism of Action in Adipose Tissue
Tesamorelin interacts directly with GHRH receptors located on adipocytes to trigger lipolysis. This process involves the enzymatic breakdown of stored triglycerides into free fatty acids for energy utilization. The resulting elevation of Insulin-like Growth Factor 1 (IGF-1) plays a secondary but vital role in reducing the volume of deep fat stores. Tesamorelin is a stabilized GHRH analogue used primarily for visceral adiposity research. Current data from 2025 indicate that tesamorelin for visceral fat studies provides a reliable model for observing non-surgical lipid reduction in complex metabolic environments.
Research Grade vs. Pharmaceutical Grade
Distinguishing between laboratory-grade compounds and pharmaceutical products is necessary for regulatory and scientific compliance. Research-grade peptides are intended specifically for in vitro and in vivo study within controlled environments. High purity standards are the benchmark for peptides Australia researchers require for peer-reviewed validation. In 2026, Australian laboratory standards demand a minimum purity of 98% to ensure results aren't skewed by manufacturing byproducts.
Sourcing from reputable Australian suppliers ensures that chemical assays remain consistent across multiple trials. Research budgets in Australia for 2026 often allocate upwards of A$450 per batch for high-purity compounds to protect experimental integrity. This precision is vital when calculating micro-dosages or observing cellular responses in sensitive adipose tissue models. Using lower-tier substances can introduce contaminants that interfere with IGF-1 signaling data.
The Pathophysiology of Visceral Adipose Tissue (VAT) in Metabolic Research
Understanding the distinction between Visceral Adipose Tissue (VAT) and Subcutaneous Adipose Tissue (SCAT) is critical for modern metabolic research. SCAT resides directly under the skin and serves as a relatively stable energy reservoir. In contrast, VAT is a pathogenic fat depot located deep within the abdominal cavity, where it surrounds vital organs like the liver, pancreas, and intestines. By 2026, scientific consensus has shifted away from using total Body Mass Index (BMI) as the definitive health marker. Instead, researchers prioritise the VAT-to-SCAT ratio, as excess visceral fat is the primary driver of metabolic syndrome and systemic inflammation.
Current tesamorelin for visceral fat studies emphasise the importance of selective lipolysis. Unlike traditional weight loss methods that often result in the loss of both fat and lean muscle mass, peptide research focuses on reducing ectopic fat while preserving skeletal muscle. This targeted approach is essential for maintaining a healthy basal metabolic rate during clinical interventions.
VAT as an Endocrine Organ
Visceral fat isn't merely an inert storage site; it functions as an active endocrine organ. It secretes a range of pro-inflammatory cytokines, including Interleukin-6 (IL-6) and Tumor Necrosis Factor-alpha (TNF-α). These substances enter the portal circulation directly, where they impair insulin signaling and promote chronic low-grade inflammation. Research models indicate that a 15% reduction in VAT can significantly improve insulin sensitivity and glucose disposal rates. Tesamorelin is specifically designed to target this tissue. It mimics endogenous Growth Hormone Releasing Hormone (GHRH) to stimulate natural growth hormone pulses. Because visceral adipocytes possess a higher density of growth hormone receptors than subcutaneous cells, tesamorelin for visceral fat studies shows a unique ability to reduce abdominal girth without affecting peripheral fat stores.
Liver Fat and Histology
The "portal hypothesis" describes how excess VAT leads directly to hepatic steatosis. When visceral fat breaks down, it releases a flood of free fatty acids into the portal vein, which drains directly into the liver. This process triggers lipid accumulation and oxidative stress within hepatocytes. Data from the Tesamorelin Effects on Liver Fat and Histology in HIV study confirmed that this peptide can reduce hepatic fat fractions by roughly 13% over a six-month period. These histological improvements are vital for preventing the progression from simple steatosis to advanced fibrosis or Metabolic-Associated Steatotic Liver Disease (MASLD).
Australian research facilities are increasingly investigating these pathways to develop protocols for metabolic recovery. Scientists requiring high-purity materials for these models can source laboratory grade compounds to ensure the integrity of their histological data. The potential to reverse early-stage liver fat accumulation represents a major milestone in 2026 metabolic research, offering a path to mitigate long-term cardiovascular risks associated with abdominal obesity.
Key Clinical Studies: Tesamorelin’s Impact on Visceral Fat and Liver Health
Clinical trials conducted over the last decade have provided a robust framework for understanding how GHRH analogues influence metabolic health. Specifically, tesamorelin for visceral fat studies has moved beyond simple weight loss metrics to focus on organ-specific fat deposition and long-term tissue integrity. Research published in 2020 highlighted a pivotal shift in how scientists view this peptide's role in treating hepatic complications. These studies demonstrated that the compound doesn't just reduce surface-level fat; it targets the deep, metabolically active lipids that drive systemic inflammation.
The data shows a consistent 30% relative reduction in liver fat among subjects treated with the peptide compared to those on a placebo. This reduction is statistically significant and correlates with improvements in overall metabolic profiles. Researchers also observed a marked decrease in visceral adipose tissue (VAT) surface area, which is a primary driver of cardiovascular risk. By reducing the volume of this fat, the peptide helps mitigate the lipotoxicity that often leads to organ dysfunction.
The MGH Study Analysis
The Massachusetts General Hospital (MGH) conducted a landmark study focusing on HIV-associated non-alcoholic fatty liver disease (NAFLD). This randomised, double-blind trial involved a 2mg daily dose of Tesamorelin administered over a duration of 6 to 12 months. The results were definitive. Beyond the primary goal of fat reduction, this NIH Study on Tesamorelin and Fat Quality found that the peptide improved the density of the remaining fat, suggesting a qualitative change in adipose tissue. Secondary endpoints were equally telling. While IGF-1 levels rose as expected due to GHRH stimulation, glucose metabolism remained stable in the majority of the cohort, addressing concerns about growth hormone's effect on insulin sensitivity.
Predictors of Response in Research Subjects
Not every subject responds to GHRH stimulation with the same intensity. Identifying predictors of response is essential for clinical accuracy. Data indicates that baseline VAT levels are the most reliable indicator of success. Subjects with the highest initial visceral fat surface area typically see the most dramatic reductions. This suggests that the peptide's mechanism is most efficient when targeting dense, pathological fat stores rather than healthy subcutaneous layers.
Baseline VAT levels directly correlate with the magnitude of hepatic fat loss.
GHRH sensitivity varies based on the subject's pituitary health.
38% of placebo subjects showed fibrosis progression compared to significantly lower rates in Tesamorelin groups.
This prevention of fibrosis is perhaps the most critical finding for long-term health. It indicates that the peptide may halt the progression from simple fat accumulation to permanent liver scarring. For researchers in Australia focusing on metabolic syndrome, these findings provide a clear data-driven path for future investigations into peptide-based interventions.
Comparative Analysis: Tesamorelin vs. Other Growth Hormone Secretagogues
Researchers evaluating growth hormone secretagogues (GHS) often prioritize Tesamorelin due to its unique specificity. While Ipamorelin and CJC-1295 offer broader anabolic applications, tesamorelin for visceral fat studies remains the gold standard. It specifically targets the VAT depot without the systemic side effects seen in wider-acting compounds. Unlike retatrutide, which acts as a triple agonist to drive generalized weight loss through GLP-1, GIP, and glucagon receptors, Tesamorelin focuses on the GHRH receptor to modulate endogenous growth hormone release. This specificity is crucial for 2026 clinical models that require metabolic isolation of adipose tissue. It's the preferred choice for investigators who don't want the metabolic interference associated with less selective peptides.
The half-life and receptor affinity of these analogues dictate their utility in the lab. Tesamorelin possesses a 44-amino acid sequence that mirrors natural GHRH, providing a high affinity for pituitary receptors. In Australian laboratory settings, the cost of high-purity Tesamorelin averages between A$120 and A$180 per 2mg vial as of January 2026. This represents a higher initial investment compared to generic GHS options, but the reduction in confounding metabolic variables justifies the expense for long-term projects.
Tesamorelin vs. CJC-1295
The primary differentiator lies in the Drug Affinity Complex (DAC). CJC-1295 with DAC has a half-life exceeding 6 days, creating a "bleed" of growth hormone that lacks the natural pulsatile rhythm. Tesamorelin mimics these pulses more accurately; its shorter half-life allows for precise control over GH levels. This makes it superior for studies requiring strict adherence to physiological GH patterns. Researchers often find that Tesamorelin provides a more predictable response in tesamorelin for visceral fat studies where hormonal spikes are a required variable.
Synergistic Research: Combining Peptides
Emerging frameworks explore combining Tesamorelin with BPC-157 to investigate systemic recovery. While Tesamorelin addresses metabolic fat reduction, BPC-157 facilitates tissue repair. Research models suggest that GH secretagogues interact with healing peptides by upregulating IGF-1, which potentially accelerates the regenerative effects of BPC-157. Multi-peptide complex research requires careful monitoring of receptor saturation to avoid desensitisation. Safety considerations in 2026 focus on ensuring that these combinations don't over-stimulate the pituitary axis during chronic administration.
For high-purity compounds suitable for comparative metabolic research, you can buy research grade peptides from a trusted Australian source.
Laboratory Protocols: Reconstitution and Handling of Tesamorelin
Precision in the laboratory environment dictates the success of tesamorelin for visceral fat studies. Lyophilized Tesamorelin arrives as a stable, freeze-dried cake. Researchers should store these vials at -20°C for durations exceeding 90 days. For immediate use within a 30-day window, a temperature range of 2°C to 8°C is sufficient. Exposure to UV light or ambient room temperature for more than 24 hours will compromise the peptide's primary structure, leading to unreliable data in 2026 research models.
Reconstitution Best Practices
Successful reconstitution requires a slow, controlled addition of a diluent. Researchers must use high-quality bacteriostatic water to ensure the compound remains stable and sterile throughout the study period. Use a sterile syringe to introduce the diluent, aiming the stream at the glass wall of the vial. Never drop the liquid directly onto the lyophilized powder. This technique prevents shearing, which is the mechanical breakdown of delicate peptide bonds. Once the liquid is added, swirl the vial with a gentle circular motion. Don't shake the vial, as agitation can cause denaturing of the protein structure. A clear, colourless solution should form within 120 to 300 seconds.
Accurate micro-dosing depends on precise concentration calculations. In typical 2026 laboratory protocols, adding 2ml of bacteriostatic water to a 2mg vial of Tesamorelin creates a concentration of 1mg per ml. This allows for increments of 100mcg per 10 units on a standard research syringe. Maintaining a sterile field is mandatory. Wipe all vial stoppers with 70% isopropyl alcohol before every needle insertion to prevent cross-contamination within the research environment.
Storage and Shelf Life
Reconstituted peptides are significantly more fragile than their lyophilized counterparts. Stability for tesamorelin for visceral fat studies lasts approximately 8 to 14 days when refrigerated consistently at 4°C. After this 14-day window, the efficacy of the compound begins to decline rapidly. Researchers should look for specific signs of degradation, such as:
Visible particulates or "floaters" in the solution.
Cloudiness or a milky appearance.
Changes in colour from a clear state.
Failure of the solution to remain fully dissolved.
If any of these markers appear, the sample is considered contaminated or expired and must be discarded. Dispose of all expired research compounds according to Australian laboratory hazardous waste regulations. Proper documentation of reconstitution dates on vial labels is a critical step for maintaining the integrity of longitudinal scientific data.
Advancing Metabolic Research Standards for 2026
The 2026 landscape of metabolic science confirms that Tesamorelin remains a pivotal tool for investigating visceral adipose tissue. Clinical data indicates this GHRH analogue can reduce VAT by approximately 18% while simultaneously improving liver fat fractions by up to 20% in specific research models. These metrics highlight its clinical significance over standard secretagogues for targeted adipose studies. Precision in laboratory protocols, especially during the reconstitution phase, is vital to preserving the integrity of these results. The ongoing role of tesamorelin for visceral fat studies continues to provide researchers with a reliable framework for understanding complex endocrine-mediated fat loss.
Peptide Research AU supports these scientific endeavors by providing laboratory-grade compounds that meet the highest industry standards. Every batch undergoes rigorous third-party purity testing to ensure your research data remains untainted and reproducible. We offer reliable, Australian-based shipping throughout 2026; this ensures your facility avoids the complications and delays of international logistics. You'll receive the exact chemical profile required for sensitive metabolic assays and longitudinal studies.
We're ready to help you achieve your next research milestone with the precision and quality your project deserves.
Frequently Asked Questions
What is the primary mechanism by which Tesamorelin reduces visceral fat?
Tesamorelin functions as a Growth Hormone-Releasing Hormone (GHRH) analogue that stimulates the pituitary gland to secrete endogenous growth hormone. This increase in growth hormone levels triggers lipolysis, specifically targeting the breakdown of lipids in visceral adipose tissue. Research indicates this mechanism is highly selective. It doesn't cause the same glucose intolerance often associated with exogenous growth hormone administration in laboratory models.
Does Tesamorelin affect subcutaneous fat as much as visceral fat?
Tesamorelin primarily targets visceral adipose tissue (VAT) and has a negligible impact on subcutaneous fat levels. In clinical trials, subjects showed a 15% to 20% reduction in visceral fat while subcutaneous fat remained largely unchanged. This specificity makes it a unique tool for tesamorelin for visceral fat studies where researchers need to isolate deep abdominal fat reduction. It doesn't affect the fat layers directly under the skin.
What did the 2020 clinical studies reveal about liver fat and Tesamorelin?
Clinical studies published in 2020, specifically those involving HIV-associated lipodystrophy, demonstrated that Tesamorelin reduced intrahepatic triglyceride (IHTG) levels by 37%. This research conducted by Takara et al. highlighted a significant decrease in liver fat content compared to the placebo group. The data suggests that the peptide's metabolic influence extends beyond abdominal fat to include organ-specific lipid deposits.
How is Tesamorelin typically reconstituted in a laboratory setting?
Researchers typically reconstitute Tesamorelin using 1 mL to 2 mL of bacteriostatic water or sterile saline solution. The process involves gently swirling the vial until the lyophilized powder completely dissolves into a clear liquid. You shouldn't shake the vial because vigorous movement can denature the peptide structure. Precision in this step ensures the compound remains viable for accurate experimental results.
What are the main differences between Tesamorelin and CJC-1295 for research?
The main difference lies in specificity and half-life. Tesamorelin is a 44-amino acid peptide specifically studied for visceral fat reduction, whereas CJC-1295 is often modified with DAC to extend its half-life to 6 or 8 days. Tesamorelin has a shorter half-life of approximately 26 to 38 minutes. This requires more frequent administration in research protocols to maintain consistent growth hormone stimulation.
Can Tesamorelin be used for research into non-alcoholic fatty liver disease (NAFLD)?
Tesamorelin is currently a primary focus for research into Non-Alcoholic Fatty Liver Disease (NAFLD) and Non-Alcoholic Steatohepatitis (NASH). A 2020 study showed it prevented the progression of liver fibrosis in 35% of participants. Researchers use it to explore how increasing endogenous growth hormone can reverse hepatic steatosis. It's a critical compound for investigating metabolic liver disorders in controlled laboratory environments.
What is the stability of Tesamorelin after it has been mixed with a diluent?
Once mixed with a diluent, Tesamorelin remains stable for approximately 24 to 48 hours when stored in a refrigerated environment between 2 and 8 degrees Celsius. Some laboratory protocols suggest using the solution immediately to ensure maximum potency. It's essential to keep the reconstituted peptide away from direct light. Extended storage beyond 48 hours often leads to degradation of the peptide chains.
Are there specific IGF-1 monitoring requirements in Tesamorelin research?
Researchers must monitor Insulin-like Growth Factor 1 (IGF-1) levels because Tesamorelin consistently elevates this biomarker. In standard research protocols, IGF-1 levels are checked every 3 to 6 months to ensure they remain within a safe physiological range. High IGF-1 levels can indicate an excessive response to the GHRH stimulation. Monitoring provides essential data on the efficacy and safety profile during tesamorelin for visceral fat studies.



Comments